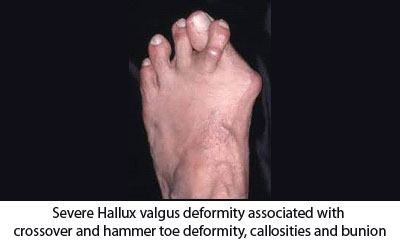
Hallux valgus is the deformity of great toe in which it deviates towards the lesser toes and the joints between the toe and foot becomes prominent, red and painful. On common man’s it has been called as bunion meaning bony prominence of inner aspect of base of hallux. But it is a misnomer. It’s a complex deformity involving not only the great toe but also other toe and foot bone. Most of the time it is associated with hammer toe deformity of second toe, metatarsalgia, callosities over interphalangeal joint of second toe and planter aspect of other metatarsal head.

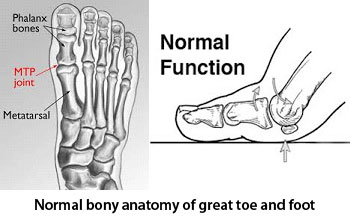
Great toe is formed with two small bone named phalanx and other toes formed with three phalanx bone. All phalanxes form synovial joint between them and also with metatarsal bones of foot. On the sole aspect near great toe below metatarsal there are two small pieces of bone are there, named sesamoid. Sesamoid helps in weight bearing during push off.
Hallux valgus can be seen in all age group and gender but it is more prevalent in female. There is a strong familial predilection of the condition. Nearly 70% of hallux valgus has a family history. It can be seen among siblings and descend among generations.
hallux valgus has two form of presentation
There are few risk factors for developing hallux valgus. Most of these factors are intrinsic, means there are some inbuilt structural abnormalities present which determines the development of hallux valgus, like
The extrinsic factors are prolonged wearing of high heel and narrow toe box shoe.
First and prominent presentation of Hallux valgus is visible deformity of great toe. Most of the time it is asymptomatic or cause mild symptom like pain and irritation at bunion site while wearing tight shoe, pain at ball of great toe and lesser toe. People who use open shoe and sleepers most of the time do not complain much from this. In severe deformity it become more symptomatic due to pain full callosities at medial border of great toe, dorsal aspect of second toe, planter aspect of lesser toe, painful bursa at bunion and arthritic changes of hallux joint.
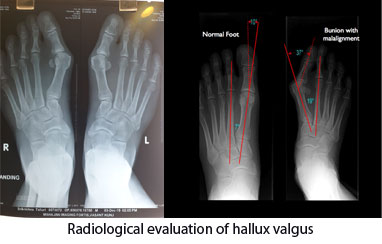
Clinical examination by the specialist foot and ankle surgeon is the key in diagnosis and determine the symptom cause of hallux valgus. 3D foot scan and foot pressure mapping are helpful in corrective insole making by detecting the pressure points deformities. Weight bearing x-ray is required to calculate amount of deformity and detect predisposing anatomical factors for developing hallux valgus as well as rule out arthritic changes. It helps in decision making for different surgical option appropriate for the specific individual.
Treatment for hallux valgus is mostly conservative with changes of foot were, using splints, cushions and corrective offloading insoles. Surgical correction of deformity for cosmetic purpose is not recommended. It is recommended only in severe juvenile type deformity and in symptomatic adult onset hallux valgus where other measures have failed to resolve the symptoms.

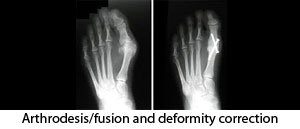
There are two main type of surgical procedures are done for hallux valgus
Different types of osteotomy have been described for hallux valgus correction. Which procedure is recommended for whom depends on severity of deformity, predisposing bony anomalies and surgeon’s preferences. Different surgical procedure can be recommended and successful for a similar deformity depending on the skill and preference of the surgeon.