


Low back pain is one of the top 10 reasons patients seek care from a Doctor. Remains one of the communist air vents for which patients come to the Orthopedic clinic. In some of the prevalence studies of different populations, the prevalence of low back pain has varied from 7.6 to 37 percent. Peak prevalence is in the group between 45 and 60 years of age, although back pain is also reported by adolescents and by adults of all ages. There is no doubt that the incidence of low back pain is increasing and as per the normal statistics each and everyone of us will have some element of back pain in our lives.
The commonest site of pain is the waist area over a wide area around the lumbar spine. Very rarely do people localise it to a small area in the lumbar spine.
There are different theories why people get back pain But there is no doubt that our posture, our way of living and our daily activities are huge contributors to the high number of patients presenting with this complaint.
The presentation is the Lake aggravated by women specially bending forward prolonged periods of setting causes a lot of stiffness and difficulty in getting up . most people are comfortable walking around and stretching . Sleep is Mukesh Lee disturb and initial waking up time is quite painful The lower back pain normally is dullish and associated with stiffness ...
hey investigations are normally not required in the initial. And clinical evaluation is enough to start the treatment . hey certain red flags which are often quoted as requiring investigations are However, the history and physical examination may elicit warning signals that indicate the need for further work-up and treatment. These “red flags” include a history of trauma, fever, incontinence, unexplained weight loss, a cancer history, long-term steroid use, parenteral drug abuse, and intense localized pain and an inability to get into a comfortable position.. . .
Some patients have symptoms primarily in the back that suggest neither nerve root compromise nor a serious underlying condition.1 Mechanical low back pain is in this category. These patients also usually improve with conservative treatment.
With this clinical classification, the examiner can use the history and physical findings to specify the type of back pain affecting the patient and properly treat patients who have potentially serious spinal conditions.
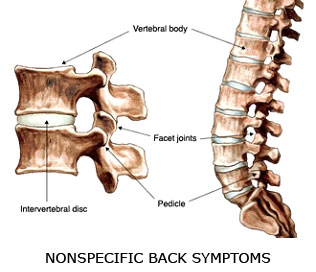
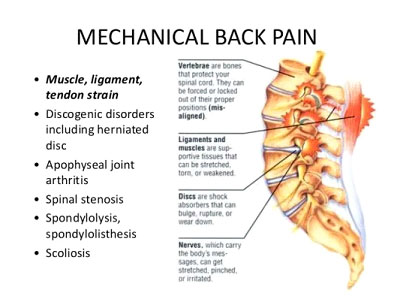
The diagnosis of low back pain requires a careful history to determine whether the causes are mechanical, or secondary and more threatening. Mechanical causes of acute low back pain include dysfunction of the musculoskeletal and ligamentous structures. Pain can originate from the disc, annulus, facet joints and muscle fibers. Mechanical low back pain generally has a favorable outcome, but back pain with a secondary cause requires treatment for the underlying condition.
Fortunately, secondary causes of low back pain are much less frequent than mechanical causes. An important consideration in the patient's history is age. Patients older than 50 and younger than 20 are more likely to have secondary causes. Clinical findings that may indicate an underlying disease are listed in Table 1.
Less common secondary causes of acute low back pain include metabolic diseases, inflammatory rheumatologic disorders, referred pain from other sources, Paget's disease, fibromyalgia and psychogenic pain8,9 (Table 2).
Adapted with permission from Deyo RA, Diehl AK. Lumbar spine films in primary care: current use and effects of selective ordering criteria. J Gen Intern Med 1986;1:20–5.
Primary mechanical derangements
Most patients require only symptomatic treatment for acute low back pain. In fact, about 60 percent of patients with low back pain report improvement in seven days with conservative therapy, and most note improvement within four weeks.14 Patients should be instructed to watch for worsening symptoms such as an increasing loss of motor or sensory functions, increasing pain and the loss of bladder or bowel function. Should any of these occur, the patient should undergo further evaluation and treatment immediately, with weekly follow-up.
Patients should gradually return to their normal activities, as tolerated. Continuing ordinary activities within the limits permitted by pain leads to a more rapid recovery than either bed rest or back-mobilizing exercises.
Patients with acute low back problems benefit from exercise programs, if started early and if the exercises cause minimal mechanical stress on the back. The goal of an exercise program is, first, to prevent debilitation related to inactivity and, second, to improve activity tolerance and return patients to their highest level of functioning as soon as possible.
Medications commonly used for the treatment of acute low back pain include aspirin and other nonsteroidal anti-inflammatory drugs (NSAIDs), acetaminophen and, possibly, muscle relaxants. Patients taking opioid analgesic drugs, often used in the first few days after the development of acute low back pain, do not return to full activity sooner than patients taking NSAIDs or acetaminophen.16 Muscle relaxants are more effective than placebo but no better than NSAIDs in relieving acute low back pain. Oral corticosteroids and antidepressants do not appear to be effective in patients with acute low back pain, and their use is not recommended.
Spinal manipulation has been shown in several randomized trials to be beneficial.17 Shoe insoles—over-the-counter foam or rubber inserts and custom-made orthotics—may also be beneficial in some patients. Spinal traction, transcutaneous electrical nerve stimulation, biofeedback, trigger-point injections, facet joint injections and acupuncture are usually not helpful in the manaagement of acute low back pain.1 Surgery may be indicated in selected patients who are not helped by conservative treatment and who have debilitating symptoms after one month of therapy. Patients with red flags noted at the initial evaluation may be candidates for immediate surgery.



