


Osteoporosis is a condition which involves the general skeleton of the human body. It is very common and is normally noted only after the age of about 60 years. Women are much more predisposed to it than men. It is also called as the “silent disease” because at most times people are not even aware of their weak bones until the end up having a fracture. The incidence of this in the Indian sub population is much more than the western population. Some of this may be related to are genetic pool but also the lack of physical activity predisposes us to this condition.

Model showing internal structure of normal & osteoporotic bone
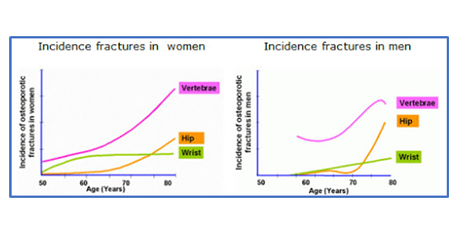
Incidence of different osteoporosis related fracture
Clinical Presentation: Most of the people with this condition present with sudden severe pain in the back or sudden pain in the wrist or hip or ankle after a relatively minor fall. Some of the people however also come with sudden sharp pain on just coughing or sneezing or even turning in bed. It causes marked difficulty in walking or moving around. These are cases of severe osteoporosis. Mild osteoporosis may not be symptomatic or may present with vague generalised bone pain, body ache or low back ache. These group of people usually get diagnosed during routine check-up. The commonest fractures that people present with are, fracture of the hip, fracture proximal part of humerus, vertebral fractures and wrist fractures.
The classical presentation of these is fracture after a fall from standing height. Once a patient with this condition is diagnosed it is understood that he or she has Osteoporosis and will require treatment.
Investigations: Include evaluation of the bone biochemistry which is done by blood test. Also, a DEXA scan of spine and maybe screening X ray of the Dorsal Spine. The scan is required to give an idea about the extent of bone weakness and may also help guide as to which pharmacological agent would be required to read this. One should always be wary in the elderly age group that any chances of any sinister illnesses such as a cancer that is spread to the bones or primary problems in the bone such as multiple myeloma has to be ruled out. One also needs to be sure that there is no long-standing kidney disorder which might have caused this problem.
CT and MRI scan have been noted to be helpful for assessing how old the injury is, and also ruling out other pathologies which could have caused the problem such as TB of the spine or multiple myeloma.
Clinical evaluation: Checking the area of pain to a certain whether this is a new injury or an old injury which is causing the problem. Specific areas of pain are identified by palpating all the spine. Patients are not always able to localise it but pressure on these areas is very helpful for assessment.
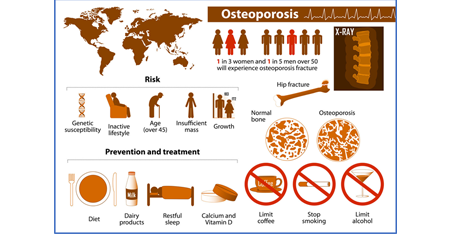
Pictorial understanding of osteoporosis
Treatment: Treatment of osteoporotic is a lifelong affair as no drug agent can actually escalate the bone density dramatically and after cessation of the medicine, bone density anyway tends to fall rather quickly. The care of these patients are essentially identifying the high risk group of population who may develop osteoporosis and to be managed by seeing them regularly and monitoring their bone density through the use of DEXA scan. One must also talk about increasing level of physical activity and also increasing the protein intake to stimulate bone formation.
The high-risk patients for this category are:
The initial treatment of osteoporosis is starting Calcium and Vitamin D medication but alone these will not cure Osteoporosis. There are essentially 3 medicine subgroups which are available for managing this condition; Bisphosphonate, Denosumab and Teriparatide a fraction of parathyroid hormone.
Bisphosphonates: This was for years the largest prescribed medication for mild to moderate Osteoporosis. These can be given in the form of tablets or even injectables. The tablets available are Alendronate, Risedronate, Ibandronate. The injectable member of this family is Zoledronate. In most people Zoledronate which is given as 5 milligrams intravenously over half an hour taken every year for 4 to 5 years has been shown to give decent results. Its action essentially is to stop the process of resorption of the bone and allows normal bone formation to keep happening at its normal pace. It is not a very strong agent for bone regeneration and needs to be given carefully in the elderly specially if they have altered renal function.
Denosumab: This is given as 6 monthly injection given under the skin in the abdomen or in the thigh. The dose of this is 60 milligrams every 6 months but should ideally be taken lifelong once started. There are very few side effects noted with this medication.
Teriparatide: Possibly the strongest agent for Osteoporosis treatment presently available. This is given as a once-a-day injection underneath skin and taken for about 2 years. It acts by stimulating bone formation and not having any effect on bone resorption. It can also help in healing of fractures in case they are going into non-union. The injection is normally self-administered by the patient them sales after demonstration of the procedure by their representatives of the company or our medical staff. It however can be given at 1 stretch only once in a lifetime. There is a lot of research pointing to excellent results with all the above 3 medications.
Treatment of osteoporotic fracture initially involves management of the acute pain which might have developed. This would involve giving suitable analgesia along with cold packs and rest in the form of immobilization in braces or splints. Eventually restoration of anatomy and the normal shape of the bone will always give better results in the long term. Different bones required different treatment, but new advances have made the treatment much easier compared to before.
For the vertebral fractures good option is insertion of bone cement into the bone after making space for the bone cement through balloon inserted into the vertebra. This is done through a small incision on the back which can be done either under sedation or as a local anaesthetic procedure. The balloon is inserted into the bone, it is then distended with water to recreate the shape of the vertebral followed by insertion of cement after removal of the balloon. The procedure itself is called Kyphoplasty. The patient is allowed to walk almost immediately after the procedure and can be discharged on the same day. Sometimes a kyphoplasty may not be enough and insertion of screws and rods to hold the board may be required.
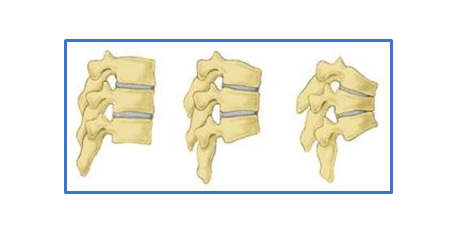
Picture showing normal vertebra and collapsed vertebra due to osteoporosis
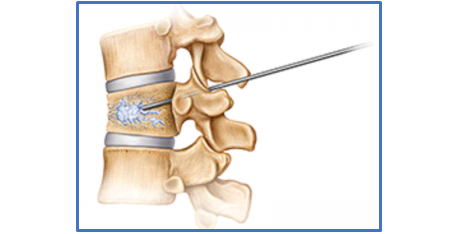
Kyphoplasty technique
For the hip fractures there are 2 common pattern are seen; intracapsular fracture neck of femur and intertrochanteric fractures. Both of them are managed with operative intervention in almost every time. The fracture neck of femur around the hip on many occasions requires replacement by insertion of an artificial hip. This procedure is called Bipolar hemiarthroplasty or Total hip replacement. The intertrochanteric fractures are treated with plate placed side of the bone or a long nail inserted within the femoral canal with screw going into the head of the femur. In both cases the attempt should be to mobilise the patient early so that they can resume at least some normal activities. All the patients initially walk with a walking frame or crutches initially almost within a day of the procedures before returning to unaided walking.

Fig: Pictorial representation of fracture neck of femur and Bipolar Hemiarthroplasty
For fractures of the wrist very often a plate may be required or on many an occasion cast can also be given to hold the fracture till it unites. The new generation of plates are wonderful, and they allow fixation of screws even in very weak bones. These newer implants are called as locking plates and have been used in our practice for over 10 years now.
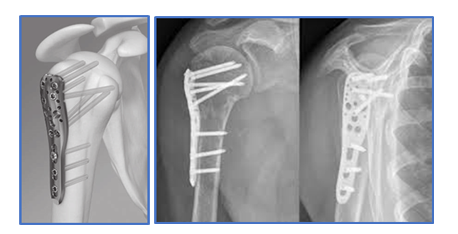
For fractures of the top end of the humerus also called as proximal humerus both options of operative and non-operative treatment can be utilised. It really depends on assessment of the fracture configuration that decision can be made to this extent.
Ankle fractures requires open reduction and insertion of plate and screws to hold the fracture
Treatment of these factures is very essential and very important for future prognosis. Every patient must understand that getting one fracture increases the chance of getting another fracture by a multiple of 2.5 times after 2 fractures the chances of getting another fracture multiplies by about 5 to 7 times. Fixation of one fracture does not in any way imply that another fracture will not be seen in the very near future.
Hey regular follow up in orthopaedic clinic or endocrinology connect is helpful in management of this condition which can be very disabling and vocationally life threatening.



