


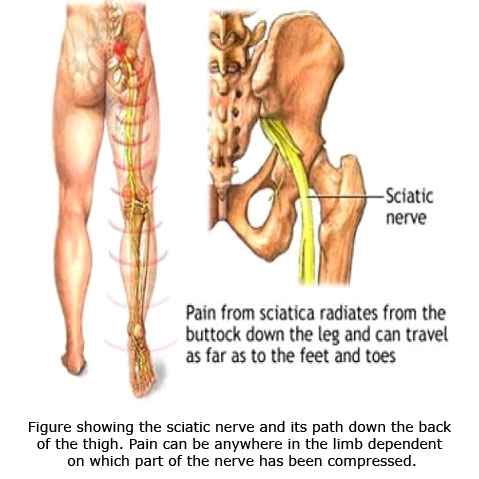
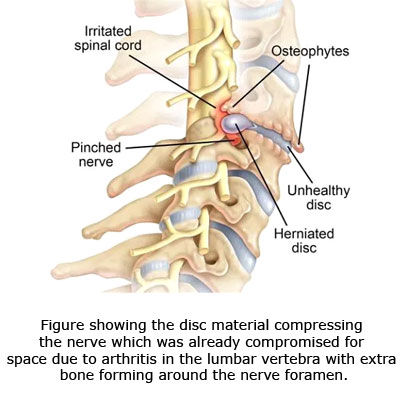
This is a fairly common problem noted in everyday Orthopedic practice. People complain of shooting pain which travels down from the back into the buttock and normally along the outer side of the thigh to any part of the leg .The common is cause for this is compression Of the nerve in the vertebral column . The commonest cause of pain in the vertebral column is a disc which is protruded backwards and is now irritating the nerve. Pain can be quite severe and even sometimes noted at rest. Patients describe the pain differently from a burning pain to a feeling as if somebody is stabbing them in the thigh or the back.
The first episode may be precipitated by simple activities such as bending down to pick up a suitcase or sometimes even picking a fallen Pen or pencil. Some people complain of pain when they bent down to rinse their mouth and then felt a sudden jab of pain in the back after which they could not straighten their back.
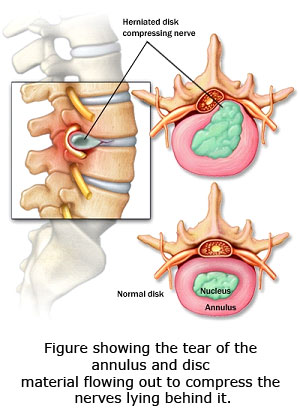
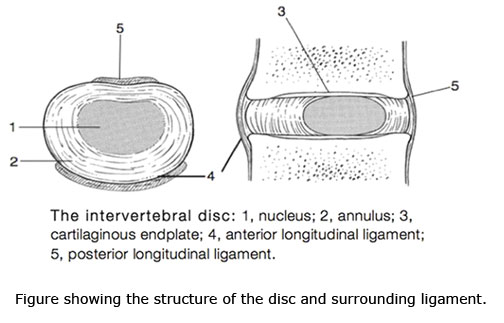
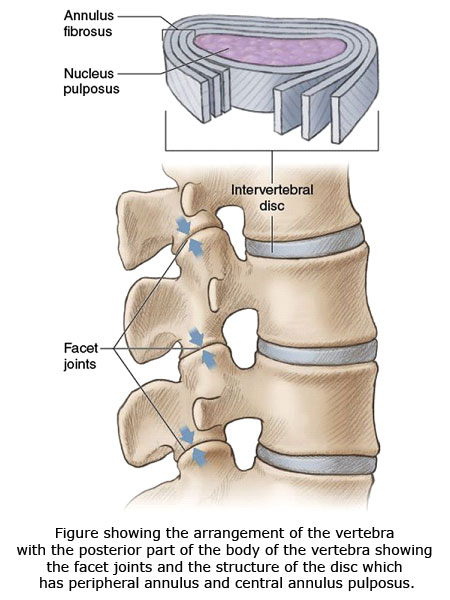
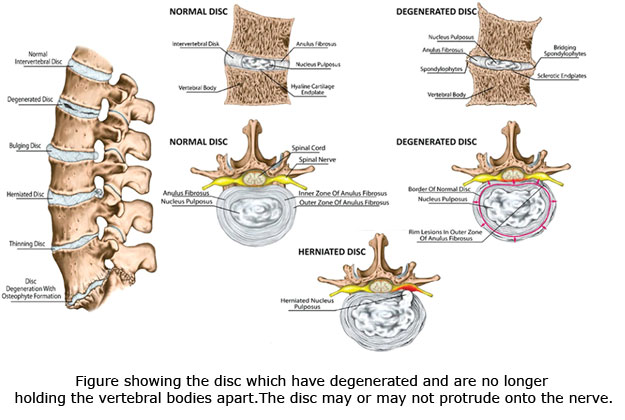
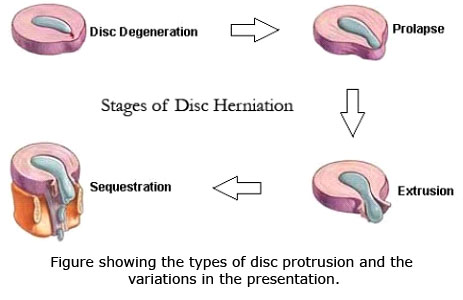
The disc is a soft structure sandwich between 2 hard bones. Its outer margin is call the annulus fibrosis and is a tough ligament which surrounds that disc and gives it a shape. The disc itself is a soft gelatinous structure which is very cushiony and has a high water content which gives it a balloon like consistency. The problem starts with the annulus getting ruptured and the disc material flowing out from the ruptured part of the annulus. In the elderly the disc itself can get degenerate on its own and become papery or wafer thin without its usual consistency and shape. In the young adults however the tear of the annulus is a precipitating factor in majority of cases.
Clinical findings normally are well localised pain which travels in one line. Severe stiffness with lack of mobility of the lumbar spine. Well localised area of tingling numbness or even heaviness in the legs. Sometimes when the pressure on the nerve is significant it might completely stop working causing significant weakness of some muscles in the leg. Very occasionally there might be complications arising from the nerves which supply the urinary bladder causing retention of urine and lack of sensation of bladder filling. This is called as a cauda equina
The disk compression can even present in a chronic way which is to say longstanding intermitted recurrent pain going down to the legs. The presentation may be very subtle in this and may have recurrent episodes of pain which seem to improve on their own after a few days.
Clinical examination: Patients often have difficulty on elevating the leg as it causes increased stretch on the nerve also called as SLR test. Evaluations of the patient should involve a full neurological assessment to look at the amount of deficit which is there as this might be one of the determinants to check for hey an indication for surgery. if significant nerve deficit is present the urgency of surgery increases as their nerve does not respond very well to prolonged compression. Manual compression on the vertebral body is often painful. Normally there is no deformity present in the vertebral column. Areas of numbness should be clearly delineated and marked out as this will indicate as to which nerve has been compressed or involved with the disc.
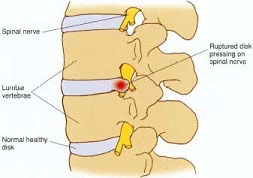
Investigations can be done in the form of an X ray which may be completely normal or should show some reduction in the disk space. MRI scans are diagnostic but are not always required as the condition can be well diagnosed based on the clinical presentation that the patient comes to the doctor with. The MRI scan will show the disk which is moved out of its place and lying very close to the nerve root. The amount of compression sometimes seems to correlate with the symptoms that the patient presents with. Sometimes the disc fragment can be separated out from its main body and an extruded fragment might be seen lying in the spinal canal where the normal nerve roots lie. The disc itself can be lying within the canal or in the outer side of the canal or sometimes in the foramen through which the nerve leaves the vertebral column.

One must also be aware of other causes off impaired nerve function such as happens in Neurological problems and also compression of the nerve from causes such as slipped vertebra, as in a condition called Spondylolisthesis. Sometimes Tumours arising from the nerve or even compression of the nerve because of fractures or compressed bone can cause similar problems. The nerve can be compressed in the pelvis by a muscle which is called as Piriformis syndrome.
Treatment the initial treatment normally is non operative and involes medications such as anti-inflammatory tablets such as Diclofenac, Ibuprofen,Piroxicam etc . This along with the nerve pain medication such as Pregabalin or Gabapentin can also be used. In addition of cold or hot compress as the patient might find useful can be prescribed. The role of bed rest is this condition is now debatable with studies not indicating to any significant advantage of prolonged period of bed rest. Patients are hence allowed to mobilise within limits of their pain but avoid certain activities such as lifting weights bending down or sitting at one place continuously for a long time. Very often the pain control can be increased by adding some synthetic opioid derivatives. Physiotherapy can be tried after a few days if the medication alone is not working.
If no relief is found after a certain time then further investigation would be required and future course of action can be made based on the MRI scan findings.
If required injection of steroids in the region of the nerve compression can be done which is a local anaesthetic procedure and is done with the 2 to 3 hours admission in the hospital. It might take quite a few weeks for the pain to settle down Normally after an acute disc prolapse the recommendation is to wait for about 6 to 8 weeks before taking any other decision regarding plan of management.
In certain locations if pain is not settling down, Patient is developing significant neurological issues which is to say weakness or numbness in the feet or legs or if there is associated problem of the urinary bladder then an operative option might be indicated . The operation involves removing the disc through a small surgery through the back. This is now days normally done under microscopic vision through a very small incision. It is also possible to do this surgery using endoscopic means which is through the means of small scope which allow visualization of the nerve root followed by removal. The procedure can be done in a single day admission and the patient can be mobilised the very next day within limits of his pain and discomfort.
The future prognosis normally is good but the patient is asked to be cautious as regards his back in terms of activities. He is advised to stop lifting to heavy awaits and to not sit unsupported and make sure that he avoids putting too much weight. Certain activities such as lounging on the sofa or the bed are strictly disallowed and he should do some regular exercises for strengthening his core muscles and for maintaining flexibility off the back. Most people will return to full normal activity without any disability for the rest of their lives.



