The vertebral column is a weight bearing device holding the weight of the chest, the arms along with the head and transmitting it down to the pelvis through the legs. In architectural terms it is essentially a pole which is standing between the 2 weight bearing areas. The bipedal stance, which is standing on 2 legs makes this part of the human body very vulnerable to stress and forces which can cause a problem in its structural stability. When humans were primates and were taking all the weight on the 4 limbs the weight transmission in this part of the human body was not significant enough to cause problem.
The vertebral bodies depend for their stability on the core muscles of the human body which are the 1.abdominal muscles 2.the spinal muscles 3.the pelvic muscles and 4.the buttock muscles. These muscles through their contraction help the vertebra in supporting the top part of the human body. The vertebra themselves are stable because of joints between adjacent vertebra and the disc with its surrounding ligament. The disk as we have noted previously as well is prone to get disrupted from the pressure that is put on it. Destruction of the disk causes more force to be transferred to the back portion of the vertebral bodies giving rise to what is called as facetal overpressure or facetal arthritis. This facetel arthritis along with a decreased intervertebral space can cause instability in the back which can present as Spondylolisthesis or Retro listhesis.
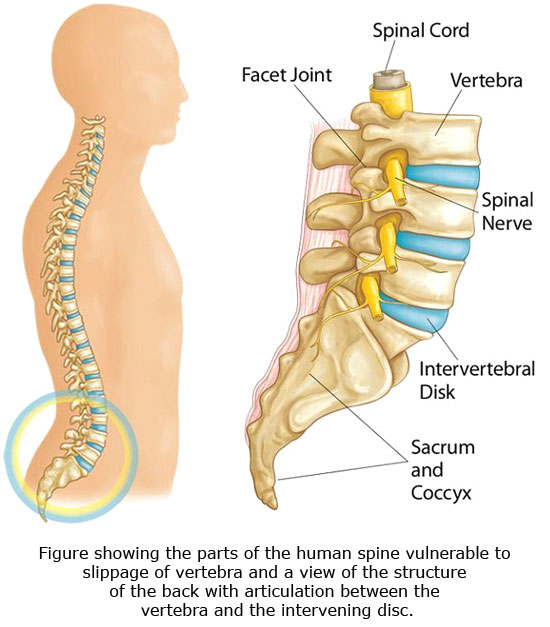
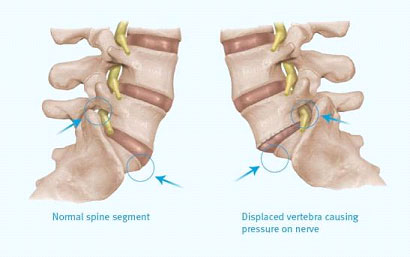
Essentially both arise from displacement of the vertebra either to the front or to the back as a consequence of the instability. There are other causes for this displacement such as 1. Post traumatic causes 2. Congenital alteration in the shape of the vertebra 3. Dysplastic causes due to malformed bones 4. degenerative causes 5. Pathologic causes secondary to infection or tumors.
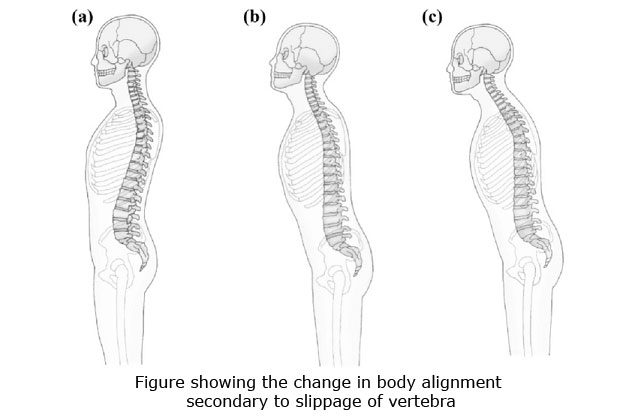
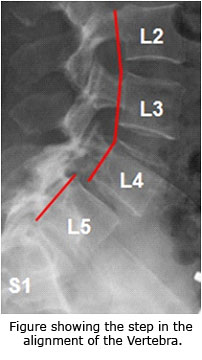
The displacement of the vertebra leads to pain in the back and an altered overall alignment of the lower back compared to the back of the chest wall and the pelvis. This may manifest even as altered pelvic alignment and eventually tightness of the hamstring muscles which are present at the back of the thigh
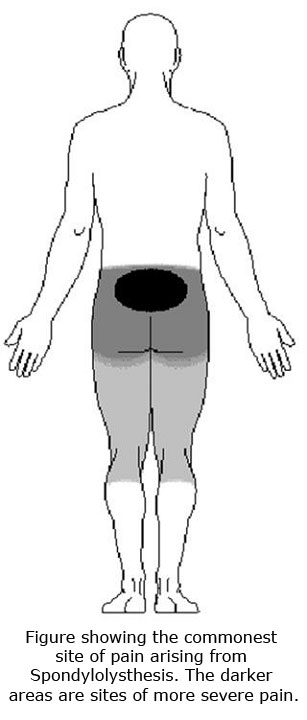
The displacement can also reduce the cross-sectional area of the foramen where the nerves exit from the spinal cord and come out from the sides of the vertebra. This causes more leg pain rather than back pain.
The symptoms are very variable and can be anywhere from occasional mild back pain and stiffness to extreme disability and difficulty in walking. The nerve can be significantly compressed to stop their working at times although not so commonly. The pain is always intermittent and does settle down in between rather than being a continuous pain.
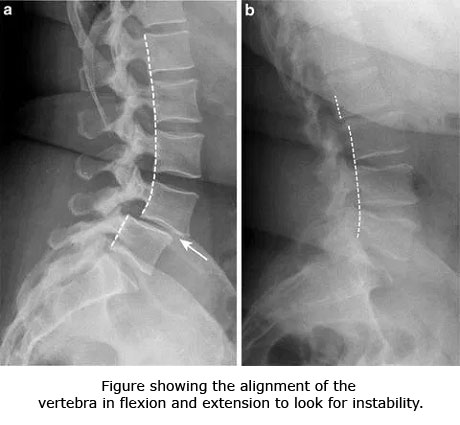
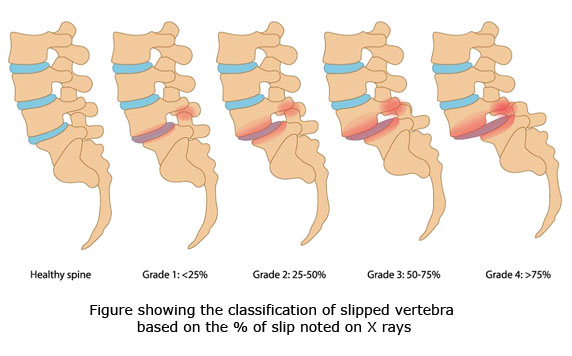
Investigations in the form of x-rays are a preliminary way to look at the problem. Normally x rays would be done from the side bending backwards and forwards to assess for displacement that takes place. These are also called as dynamic X Ray views.
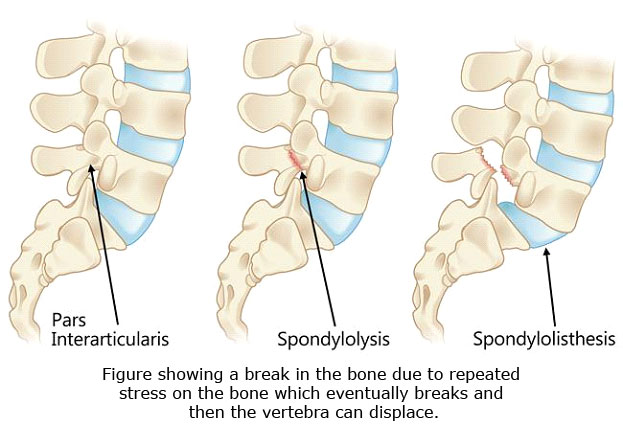
CT scan is often helpful and meshu small cracks in the boon or areas where the bone has separated out in certain types of listhesis. MRI scan is normally more useful as it can show the nerve along with compression which is there. It will also be able to distinguish whether the compression is from bony elements or soft tissue elements.
Treatment :in the beginning an attempt can be given to non-operative management in the form of exercises and occasional use of supportive braces. Change in the lifestyle especially the occupation if it involves excessive movement of the back or excessive load transmission as in manual Labour is useful but not always practical. Good posture control however and the means paramount and should be done by all people especially those in desk job hey or people working at very low levels such as plumbers and electricians. hey, many time spaces models who watch their back significantly and gymnast could extend their back backwards many many times are prone to this problem and need to be advised to take special precautions.
Can predispose to Spondylolysis. If, however the treatment has not succeeded then operative intervention remains an option. Operative intervention would depend on the cause for the slippage of the vertebra and the amount of slippage. The factors to be taken into consideration include the age of the patient, the symptoms that the patient has and the degree of neurological compression that the patient has presented with.
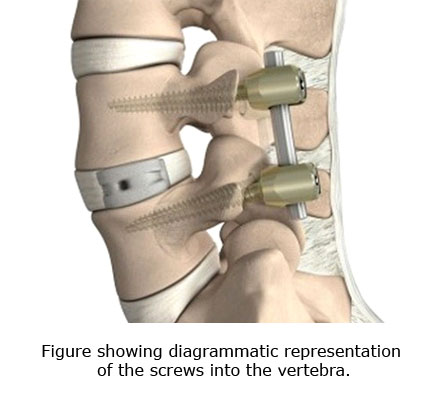
Standard surgical procedure is decompression and Fusion, which involves approaching the vertebra from the back putting screws into the bone. Pulling the bone back in into its normal position and then fusing it in the normal position to the vertebra below it. Once bone to bone union has occurred between the 2 vertebral bodies the patient can be asked to resume full normal activities