


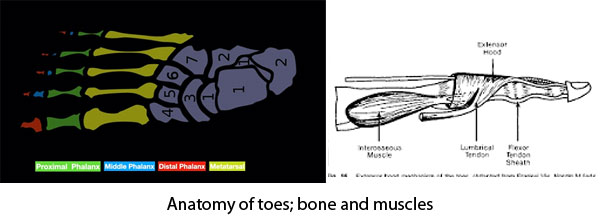
Toes assist us in balancing while standing and walking and also providing thrust during gait. Toes are consits of small bones, phalanx. Second to fifth toe have 3 phalanges proximal middle and distal where as great toe has only proximal and distal phalanx. Movement and stability of the toes are maintained by strong capsule, intrinsic muscles of foot, extensor and flexor tendons and their expansions. Chronic imbalance of these tendons along with weakness or deficiency of the capsular integrity causes development of toe deformity.
Toe deformities are present in 3 forms. These deformities are either fixed or flexible.
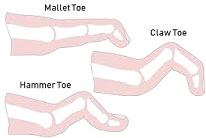

Prolong use of foot wear especially high heel and pointed narrow toe box shoe and lack of bare foot walking can cause weakness of intrinsic muscle of foot which ultimately produce imbalance of long tendon functions around toes. Wearing of a shoe with high heel and tight narrow toe box forces the toes remain buckled and curled up. In the long run these influences development of mallet and hammer toe deformity. Chronic disuse, neuropathy (DM Neuropathy) and in congenital neurological condition intrinsic muscles of foot become weak and develop claw toe deformity. Hallux valgus deformity also forces the second toe to develop complex hammer toe deformity. Long standing deformity caused friction of skin with foot wear and weight bearing area results in formation of thick painful keratinized skin these are called callosity. Common sites where callosity developed are dorsal aspect of PIP joint in hammer and claw toe deformity, at tip of the toe in mallet toe deformity and at planter aspect of ball of foot in hammer and claw toe deformity.
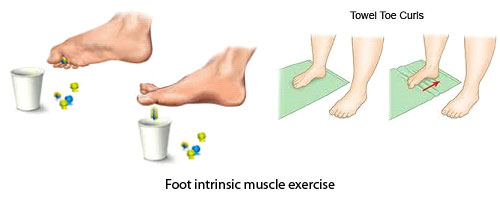
Flexible deformity and mild deformity can be managed with changes in foot wear and cushioning orthotics. Variety of orthotics and cushions are available commercially which one can use according to their comfort. Your physiotherapist or physician can also advice you regarding the choice. Foot intrinsic muscle strengthening can help in preventing toe deformity.


Severe deformity with painful callosities and ulcers requires surgical correction of deformity. Different soft tissue reconstruction procedures are also recommended in flexible deformity to prevent development of crocked deformity.




